



Plaque Regression: Can We Reverse Arterial Buildup?

Plaque in our arteries—whether in the carotids, coronaries, or even smaller vessels—remains a leading driver of heart attacks, strokes, and circulation issues. The good news? Emerging data suggests that plaque regression (actually shrinking or stabilizing plaque deposits) may be possible under the right conditions. Below is an overview of the science, key interventions, and studies that highlight how we can nudge plaque in the right direction.
1. Why Plaque Regression Matters
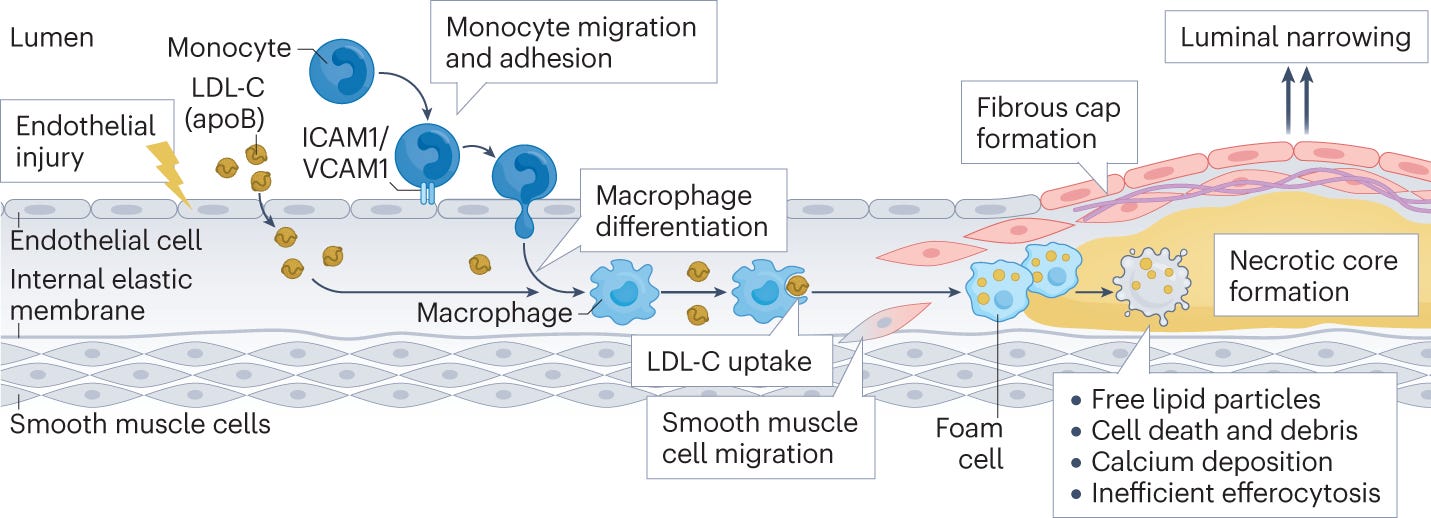
Arterial plaque (atheroma) buildup is often a slow process, fueled by inflammation, oxidative stress, and unbalanced lipids. When plaque becomes unstable or blocks blood flow, the risk of heart attacks, strokes, and other vascular complications spikes. By targeting plaque regression, we aim to:
Open up blood vessels for improved blood flow.
Reduce risk of rupture or arterial blockage.
Support longevity and overall cardiovascular health.
2. Five (Plus) Interventions That May Help Shrink Plaque
A) Niacin (Vitamin B3)
Evidence: Multiple studies, including one in Future Cardiology [1], highlight niacin’s ability to improve lipid profiles and potentially stabilize plaque. When combined with other therapies (like statins), niacin has shown synergy in reducing atherosclerosis [2].
Recommended Product: Designs for Health Niacin CRT. It’s a controlled-release niacin designed to minimize the intense flushing typical of immediate-release forms.
Dose Tips: Doses of 1,500–2,000 mg daily are often used in clinical contexts for plaque control, but start low to gauge flushing. Always consult with a healthcare provider, as niacin can affect liver enzymes and blood sugar.
B) Blood Pressure Control
Target: Aim for <120/80 mmHg. Research consistently shows that maintaining healthy blood pressure helps reduce arterial stress and fosters plaque stabilization—or even regression. Elevated BP stiffens arteries, making plaque more likely to deposit and expand.
C) Optimized Thyroid Function
Studies: Low thyroid function correlates with increased carotid plaque [3]. Another study in dialysis patients found that low T3 levels were associated with greater atherosclerosis [4].
Goal: Keep Free T3 (FT3) around 3.8–4.2 pg/mL if possible (within your lab’s reference range). Ask your doctor to check a full thyroid panel. Correcting mild hypothyroidism may help reduce plaque load over time.
D) Statins
Evidence: A variety of statins—especially simvastatin and rosuvastatin—have documented plaque regression effects [5]. By lowering LDL and inflammation, statins can stabilize and in some cases shrink atheroma.
Synergy: Pairing statins with niacin has shown enhanced plaque regression in some trials [2]. If you’re open to using a statin, talk to your doctor about which specific one might be optimal for you.
E) Ezetimibe
What It Is: A cholesterol absorption inhibitor that lowers LDL levels.
Research: The ZIPANGU study [6] showed how ezetimibe can help stabilize and potentially reduce plaque. For those who prefer not to use statins or who need extra LDL-lowering, ezetimibe can be a potent partner.
3. Other Notable Options
Pioglitazone (for Diabetics or Pre-Diabetics)
Mechanism: A PPAR-gamma agonist that enhances insulin sensitivity and exerts anti-inflammatory effects.
Study Spotlight: In a prospective study with intravascular ultrasound, pioglitazone led to regression of coronary atherosclerotic plaques in patients with type 2 diabetes or impaired glucose tolerance [7].
Caution: Monitor blood sugar and watch for fluid retention. This is a prescription drug, so discuss with your doctor.
4. Practical Strategies to Enhance Plaque Regression
Diet & Exercise: A whole-foods, balanced diet (rich in vegetables, lean proteins, and healthy fats) plus regular moderate exercise can reduce LDL, raise HDL, and promote vascular health.
Lower Inflammation: Minimizing refined carbs and sugars, getting enough sleep, and managing stress help tamp down chronic inflammation (a big driver of plaque growth).
Regular Labs & Imaging: Periodically checking lipid panels, thyroid levels, and blood pressure helps gauge progress. Some cardiologists may use ultrasound or advanced imaging to track plaque changes directly.

5. Key Studies & References
Effects of Niacin on Atherosclerosis: PMC3145140
Statin + Niacin on Plaque Stability: PMC3242018
Thyroid Function & Carotid Plaque: PubMed:18495692
Triiodothyronine Levels & Arterial Stiffness: PMC3358995
Efficacy of Statin Therapy in Plaque Regression: PMC5090812
Ezetimibe on Plaque Stabilization (ZIPANGU): PubMed:28592751
Pioglitazone & Coronary Plaque: PubMed:18817993
6. Summary & Takeaways
Plaque regression isn’t a pipe dream—it’s an evidence-based possibility. Whether you lean toward niacin (like Designs for Health Niacin CRT), or consider statins, ezetimibe, pioglitazone, or ensure your thyroid is optimized, you can create a multi-pronged plan for tackling arterial plaque. Add in consistent blood pressure control and healthy lifestyle measures, and you’ve got a powerful synergy working in your favor.
Key Steps to Consider
Get your BP <120/80 mmHg.
Evaluate thyroid status—keep FT3 near the upper normal range.
Discuss niacin, statins, or ezetimibe with your physician if your lipids or plaque burden warrant it.
Explore pioglitazone if you’re diabetic/pre-diabetic and your doctor deems it appropriate.
Remember: Always consult your healthcare provider before adding or changing any medication or supplement—especially for something as critical as plaque regression. With the right strategies, you might just see your plaque load head in the right direction—down.
Disclaimer
This article is meant for educational purposes and does not replace professional medical advice. Always consult with a qualified healthcare professional regarding treatments for arterial plaque or other cardiovascular concerns.
Statins are so vilified I have been prescribed them but as yet haven’t taken them. Such divergent opinions I don’t know what to believe